
Is there really a 400% increase in colorectal cancer incidence amongst children?
No, it was probably a ICD classification change

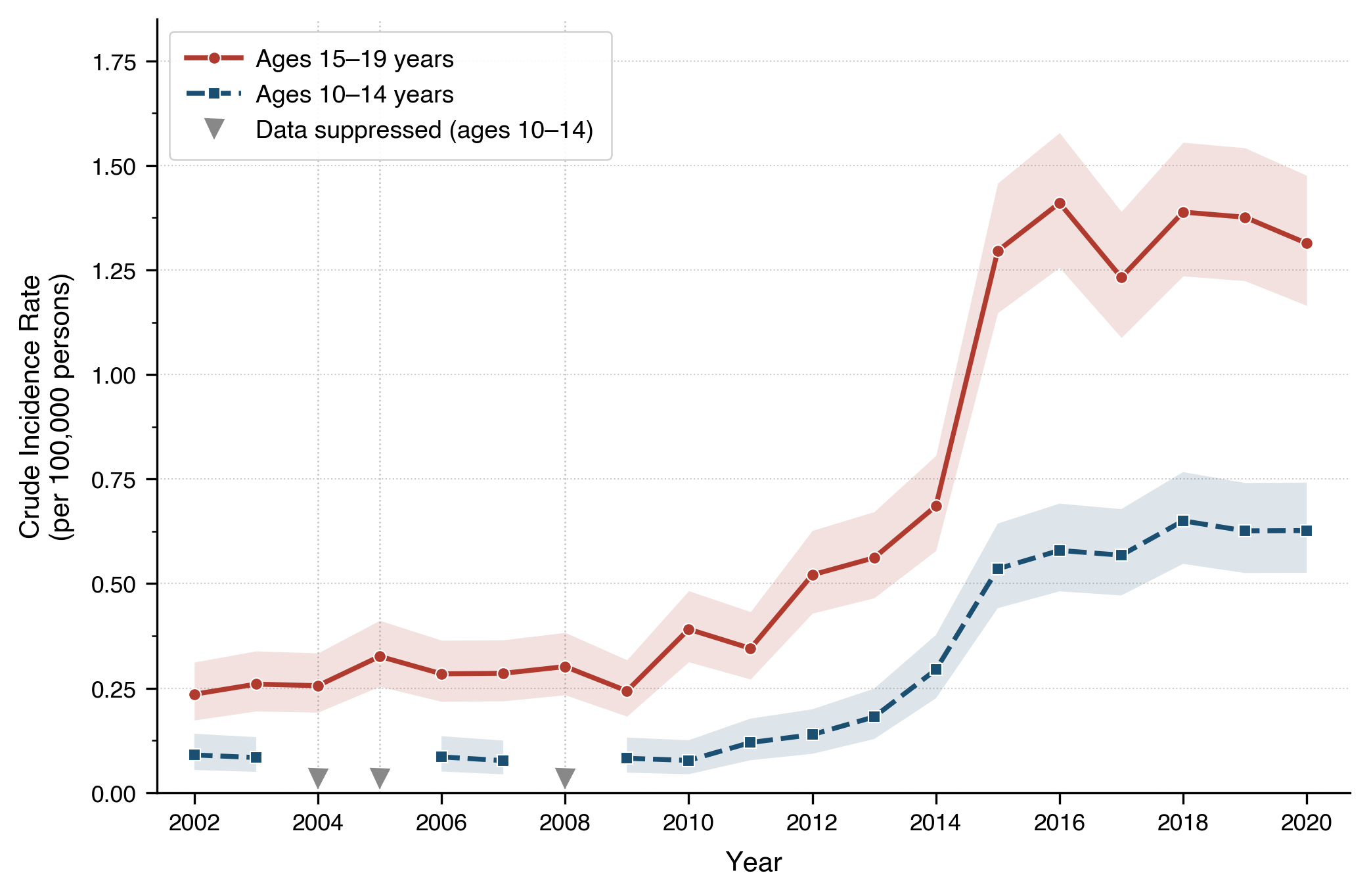
The uptick in early-onset (< 50 years old) colorectal cancer incidence has been a topic of much discussion and investigation. One striking observation is that in the US from 1999 to 2020, the incidence rate of colorectal cancers grew ~400% in individuals 10-19 years old. Decomposed by 5-year age group, we have seen a 500% increase in the 10-14 age-group and a 333% increase in the 15-19 age-group during this period. These are real numbers reported from the CDC and below are the incidence trends:
There is no consensus explanation for why early-onset CRC is on the rise. But, one theory is that early exposure to certain bacterial strains in our gut that produce toxins (e.g., colibactin) create mutations that accelerate the development of colorectal cancer. It is a popular theory that has been the subject of much online discussion. Here, I’d like to share a more plausible explanation for the rise in CRC incidence amongst the pediatric population.1
From looking at the incidence graph above, both age groups have a period of stability (roughly 2002-2012) followed by a sharp rise over the next four-ish years (2013-2016). Then, stability thereafter. Something happened around 2013. Second, we see big relative increases in the setting of low absolute counts. Note that for the 10-14 year age group, the big change happened in 2013-2015, where raw count went from 38 in 2013, to 72 in 2014, to 113 in 2015. Similarly, for the 15-19 group, the counts went from 75 in 2011 to 146 in 2014 to 277 in 2015.
If the observed stability-rise-stability pattern of CRC incidence was due to a biological process, such as exposure to colibactin, I would expect a less discrete and more gradual change in incidence rate. So, what could have happened?
We re-classified neuroendocrine tumors of the appendix as malignant.
In the second edition of the International Classification of Diseases of Oncology (ICD-O) in 1990, neuroendocrine tumors were designated as malignant for all sites except the appendix. In 2013, with the release of ICD-O-3, appendiceal neuroendocrine tumors were also considered malignant. And, the CRC incidence data from the CDC reports malignant tumors from the appendix.
Now, could this neuroendocrine change in 2013 actually produce the 10-19 year old incidence uptick from 2013-2016 that we observe?
A beautiful paper in 2025 from a team consisting of scientists from OHSU, UT, MGH, and McMaster University demonstrated that almost the entire uptick is attributable to the re-classification of neuroendocrine tumors of the appendix.
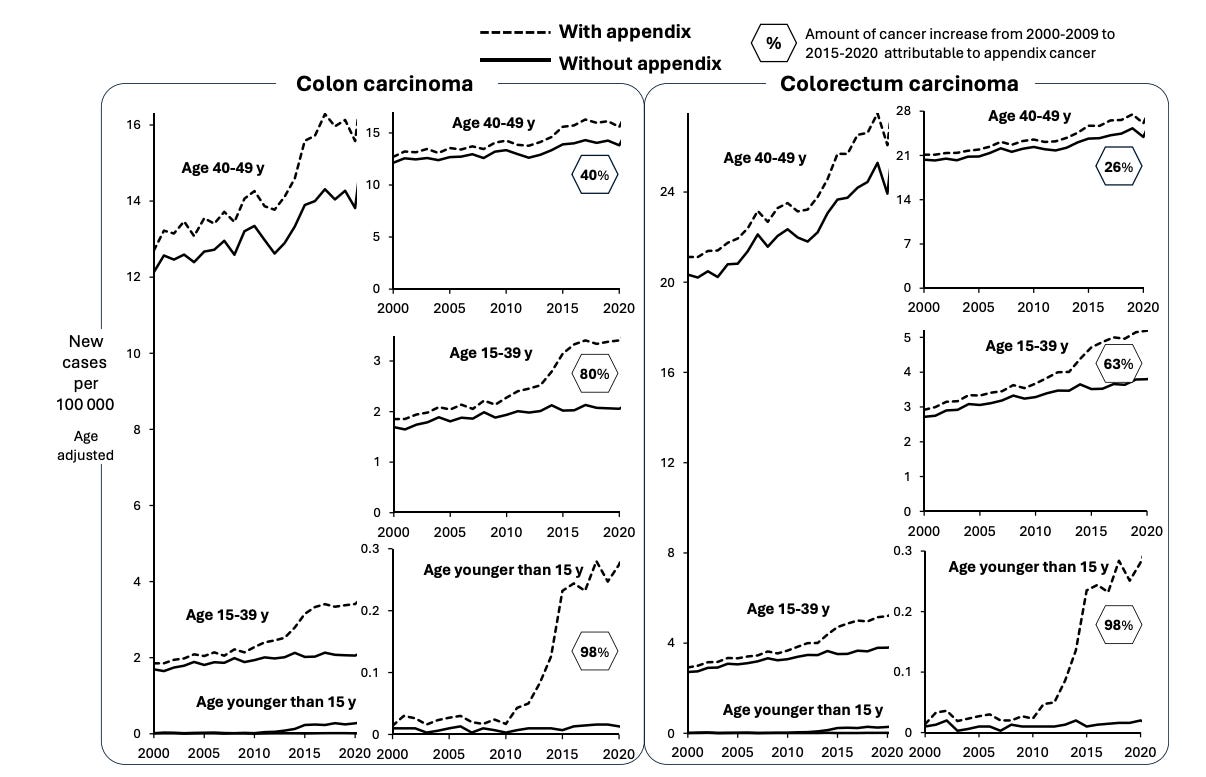
Notice that in those younger than 39, the incidence rates are basically flat before and after 2013 if we take out the appendix tumors. But, what type of appendix tumors are these?
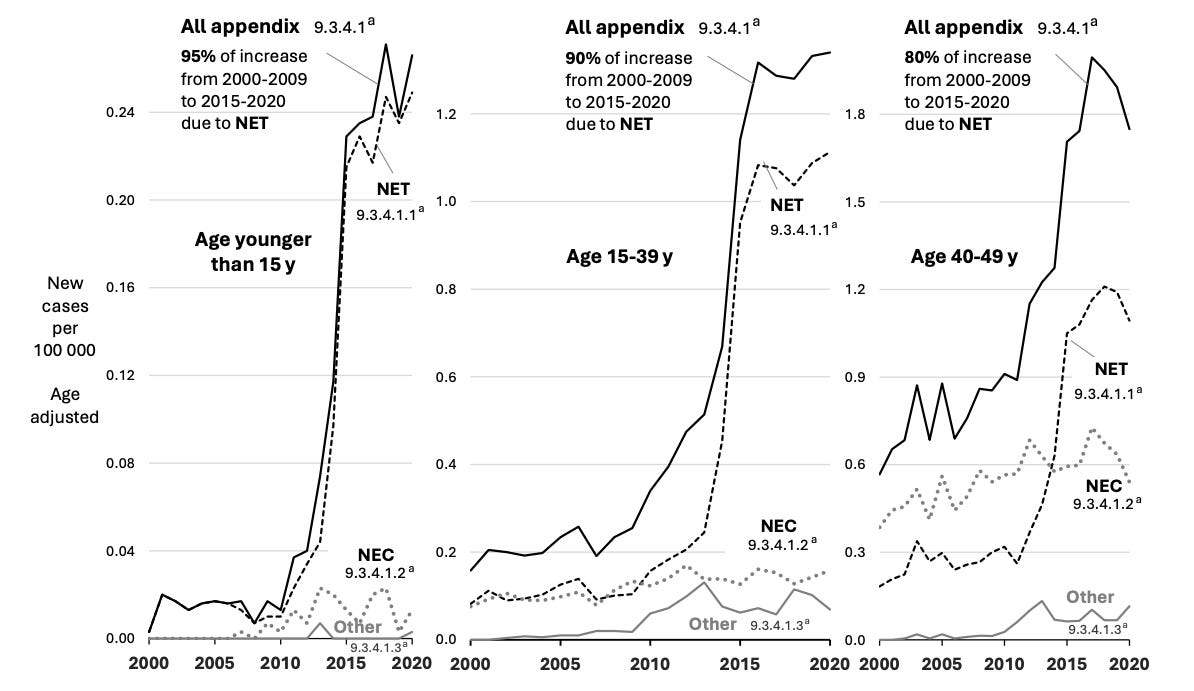
The appendix tumors are basically all neuroendocrine tumors. In the pediatric population these tumors are largely found incidentally after appendectomy for suspected appendicitis and survival is basically 100%.
This re-classification explanation is not sufficient to explain the entire uptick in individuals less than 50 years old, however. There may be a contribution from microplastics, colibactin, and lifestyle (e.g., sedentary time, ultraprocessed foods) too. An interesting consideration is that recommendations for some early-onset genetic and familial conditions that predispose people to CRC (specifically gene-specific Lynch syndrome, Peutz-Jeugher syndrome, and Juvenile Polyposis syndrome) were formalized and adopted around 2010-ish which could plausibly lead to an increase in cases in the less than 50 years old bucket. More work is needed to disentangle the contribution of these different factors.
The percent increases in incidence rate for 20-49 year olds are far lower than the 400% statistic for the teenage population. It is easier to offer explanations for things that are “outlier-esque” values.
Please see this discussion thread on X with Saloni for more color on CRC incidence rates in the US: https://x.com/salonium/status/2064901834318197020?s=20