
What do we know about the 2026 Hantavirus outbreak?
Based on all the Hantavirus data available to us

An outbreak of hantavirus occurred on the MV Hondius, a cruise ship traveling from Argentina to Cape Verde, in late April/early May. As of May 13, 11 people have been suspected or confirmed to have the Andes Virus (ANDV), a strain of hantavirus capable of human-to-human transmission. All were passengers on the cruise ship. The Brown pandemic center writes a weekly update on the situation. Click here for their May 14 update.
18 people returning back to the US are being monitored in Nebraska and Georgia but, there are a number of people who left the cruise prior to these monitoring guidelines being implemented. These folks took commercial flights back home (to all corners of the world), and sat and interacted with people on these flights and at the airports. This increases the radius of ANDV exposure. For example, an individual sitting within two seats in front of or behind an ANDV-positive person returned back to Sacramento County, where they are being monitored from home by their local public health office with check-ins and guidance to quarantine for 42 days (source). Of the 11 cases, 3 have died. One of these three individuals, prior to their death, was on a KLM flight and interacted with a flight attendant aboard the ship who fell ill shortly thereafter. This led to speculation that it could be ANDV. But, importantly, this person was ANDV-negative (both PCR and antibody) at the time of testing.
So far, there have been no cases outside people who were on the ship. The incubation period, defined as the time from virus exposure to symptom onset, for ANDV can be at least as long as 40 days. The mean incubation period in human-to-human transmission is around 23 days (~3 weeks). Practically, this means that anybody who has been exposed should not be considered hantavirus negative until 40 days after exposure. The flight attendant is negative for now but could turn reasonable turn positive until the beginning of June 2026.
Before continuing on, I should note that comments about incubation periods, symptoms, mortality rate, or anything else depend on the properties of the specific ANDV strain that is going around right now. Specifically, its RNA sequence. COVID (SARS-CoV-2) is a good recent example. If we based our assumptions of what the COVID virus in 2020 was going to do based on the SARS data from 2003, we would be wrong. SARS-CoV-2 is only about 79% similar to SARS genetically, and its genome informs its clinical properties. Further, infectivity patterns and clinical manifestations vary by strain (i.e., Delta COVID was different than Omicron). This is all to say that sequencing the ANDV strain and comparing it to the genomic data we have from prior ANDV outbreaks will allow us to understand the likely trajectory of the Hondius outbreak.
We have sequencing data from 5 patients from the Hondius outbreak. ANDV is a single-stranded RNA virus made of three RNA pieces: Small (S), Medium (M), and Large (L) segments. The M segment encodes the glycoproteins that sit on the surface of each viral particle and mediate entry into human cells. The S segment encodes the Nss protein responsible for suppressing the antiviral interferon response (source).1 The M and S sequences of the 5 Hondius-infected patients are identical and the L sequences are identical except for two synonymous mutations. Gustavo Palacios, a board member of the International Hantavirus Society and professor at Mount Sinai, notes that “the lack of [sequence] diversity observed in the outbreak is similar to that observed during a cluster of human-to-human transmission in the Epuyén 2018 outbreak, in Argentina”. Further, the S, M, and L segments in this outbreak are 98.8%, 98.7%, and 98.7% identical, respectively, to their corresponding segments in the ANDV strain from the 2018 Epuyén outbreak in Argentina (source). Clustering reveals that amongst ANDV sequences available to us, the Hondius strain is closest to samples taken from patients distinct from the 2018 outbreak in Argentina but still occurring in Argentina in 2018 which are outlined in orange in the figure below (source 1, source 2).
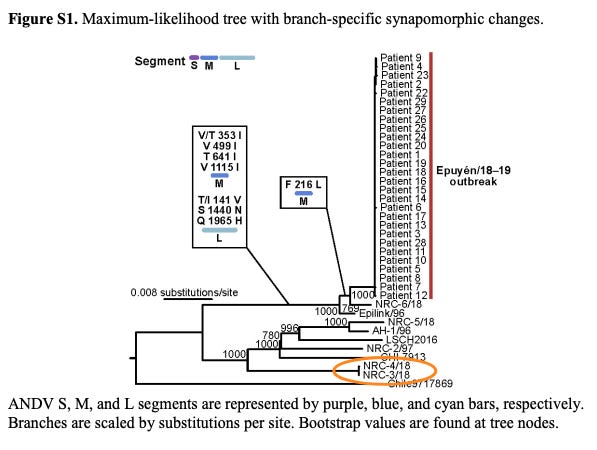
We do not have clinical data for NRC-4/18 and NRC-3/18 beyond the knowledge that they are non-Epuyen Argentinian ANDV samples taken in 2018. If we look at the clustering results from the Hondius strain, we observe that CHI-Hu13724 cases cluster near Hondius.
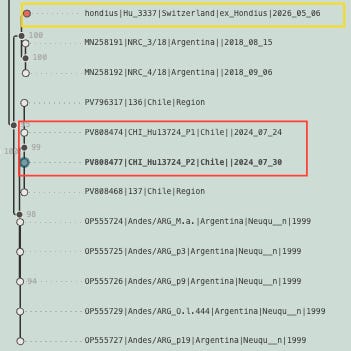
CHI-Hu13724 represents two ANDV cases in Chile in 2024 that, from what I can tell, behaved similarly in humans as past ANDV cases in the region despite differences in RNA compared to Epuyen and other case series.
During May to June 2024 in Región de los Ríos, Chile, a fatal hantavirus case of a woman and the consecutive infection of her husband led to clinical and virological follow-up of their two close household contacts, her grandson (case 136) and daughter (case 137). Nineteen days after the onset of symptoms of the primary case, case 136 tested positive for ANDV RNA by RT-qPCR in blood. The child, who remained under clinical follow-up, developed symptoms within 24 h, whereas his mother remained negative. Within the following three days, both subjects were transferred to a hospital where extracorporeal membrane oxygenation was available. After day 1 of admission, case 137 tested positive for ANDV and showed symptoms within 24 h. Both cases developed severe and mild diseases, respectively, and both survived.
Clinical characteristics appear to be concordant in the face of some differences in RNA sequences2. Therefore, it is reasonable to assume, until proven otherwise, that Epuyen and other ANDV clinical data from the region read through to Hondius clinical dynamics.
There are a few hundred cases of ANDV cases reported each year in the world, concentrated in southern South America (e.g., Argentina and Chile). Most transmissions occur from exposure to rodent (Oligoryzomys longicaudatus) feces, urine, and saliva, particularly via inhalation. Unlike other hantaviruses, ANDV is capable of human-to-human transmission.

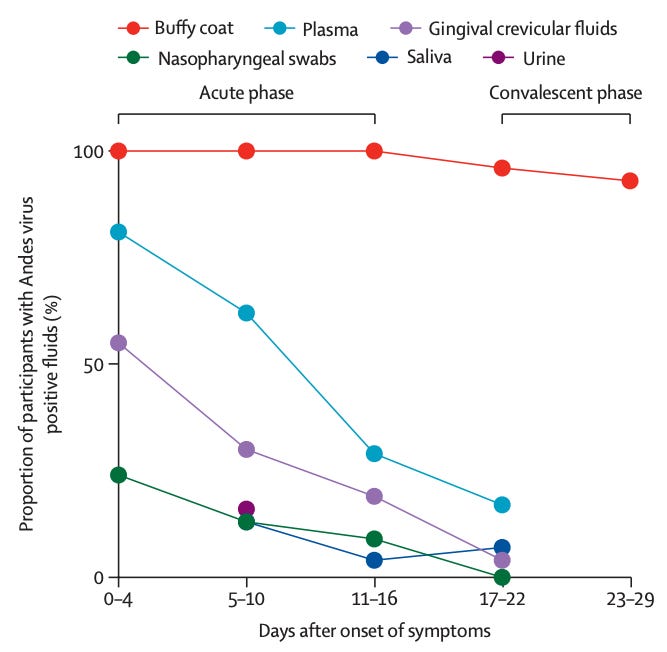
ANDV is present in blood of infected individuals up to 2 weeks before onset of symptoms, with average incubation period of 18 days albeit with high variance in time to symptom onset.3 ANDV was isolated from blood obtained from a child in Chile before the onset of symptoms or development of ANDV antibodies. Once symptoms begin, patients are ANDV positive in a range of bodily fluids although mostly in blood.
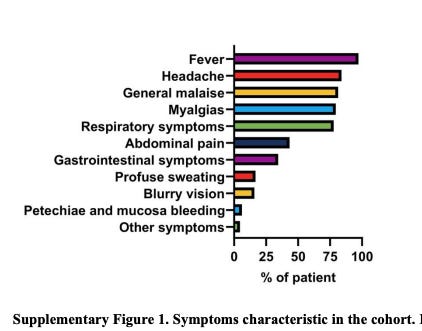
The symptoms of ANDV resemble that of the common cold, flu, or community-acquired pneumonia. The initial symptoms are non-specific and there is no tell-tale sign of ANDV. In 131 patients, these were their symptoms:
ANDV in humans can be mild (i.e., resemble the flu) or progress to hantavirus pulmonary syndrome (HPS). HPS is characterized by an initial flu-like prodrome followed by cough, shortness of breath, noncardiogenic pulmonary edema, and possible cardiogenic shock. About 20-35% of ANDV cases lead to rapid pulmonary edema followed by cardiogenic shock. Of those who develop respiratory symptoms (e.g., shortness of breath), about ~30-50% of them die (source 1, source 2).
How does ANDV spread? We will start with rodent studies then move to humans. Rodents were placed together in the same cage for 24 hours, one with ANDV positivity and the other without. Then, the initially non-positive one was quarantined for 45d. Of 130 attempts, 16 cases were recorded by seroconversion (12%). None of the 27 experiments through a wire mesh cage, resulted in infection. Only when the rodents shared a cage was there transmission. Longer range transmission is less likely than shorter range transmission which implies that modes of transmission that support longer range transmission are less effective at seroconversion. This suggests that aerosol based transmission is less effective than droplet ANDV transmission.4 This is unlike COVID where aerosol-based transmission is the dominant force.
In a 5 person case series that began from a person who was infected after rodent exposure, the other people contracted ANDV after interacting closely with the infection person. Specifically, they lived with, touched, or were around the secretions (e.g., sweat) of an infected person. Of course, the soon-to-be infected people were also within respiratory droplet or aerosol distance too. The lack of ANDV-positive patients in contacts who were only in respiratory aerosol distance (i.e., many feet away) suggests a relatively lower infectivity potential via aerosols.
The most detailed clinical characterization of ANDV is a New England Journal of Medicine paper describing the Epuyén/18−19 outbreak in Argentina. The reproductive number (R₀) is the number of secondary infections generated by a single infected individual in a completely susceptible population. The median R₀ was 2.12 before control measures were enforced. A R₀ > 1 means that each infection person creates more than one new infection, implying that the number of total infections will grow.5 In Argentina, after 18 cases and an R₀ of 2.12, they enforced isolation of ANDV-positive people, rigorous contact tracing, active clinical monitoring of close contacts, and self-quarantine of high-risk contacts. This dropped the R₀ to 0.96. In total, there were 34 cases - 33 in Argentina, 1 in Chile (after a person from Epuyén traveled to Chile) - and 11 died. 32% fatality rate was observed.
There is a general principle in virology: the more deadly the virus, the lower the R₀ (i.e., the less people it can infect). Low deadliness does not mean it can’t make you sick or leave you with lasting health problems. It certainly can. It just means most people won’t die. The Omicron variant of COVID is a high infectivity, low deadliness virus. ANDV is a low infectivity, high deadliness virus. Therefore, the probability that the Hondius strain ANDV will cause a worldwide problem on the order of the Spanish flu in 1918 or COVID in 2020 is rather low.6
We can see here that the R₀ drops after control measures are implemented along with the number of cases:
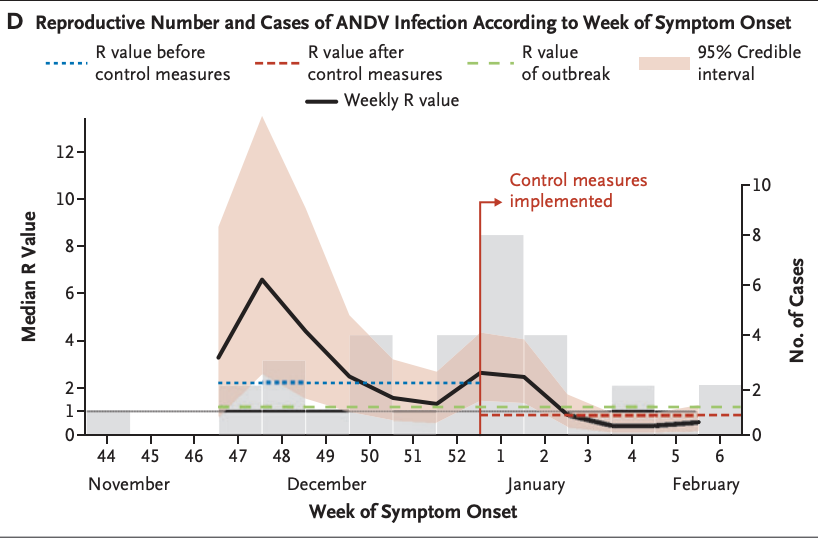
It takes about 7 weeks after control measures to get the cases down to zero. The critical difference between Epuyén/18−19 and Hondius is that the infected and exposed patients aboard the Hondius traveled to all corners of the world and sat in crowded airplanes and airports. This exponentially increases the susceptible population at risk compared to Argentina in 2018 where travel post-exposure/infection was much lower.
In the Argentina 2018 outbreak, 3 ANDV-positive patients were the source of 21 of 33 secondary cases. The first event that cause secondary infections was at a birthday party. Here is the seating chart and ANDV-status of the attendees:
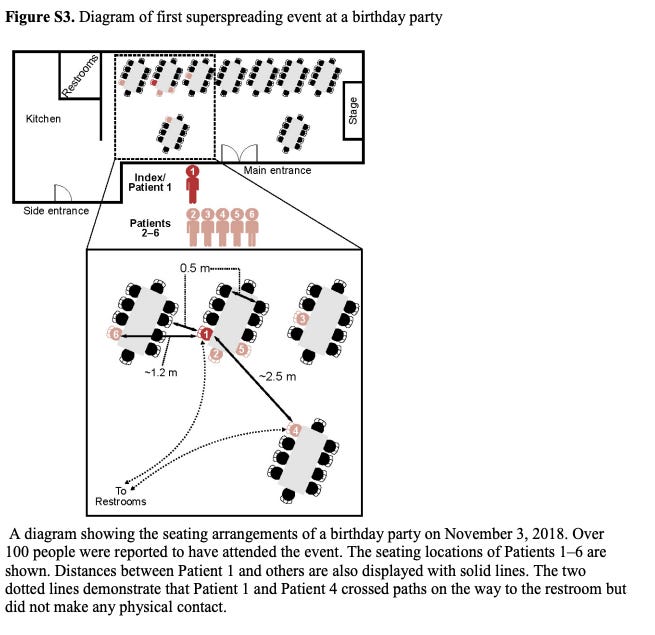
Patient 2 and 5 were sitting very close to Patient 1 (within 2 feet). There are ~4 other people seated within 2 feet of Patient 1 who did not get the virus. The infection rate within a 2 foot radius is around 33%. That’s a high rate of infection but not a gaurauntee of infection. How did Patient 3, 4, and 6 get the virus? Patient 1 is a male and so it patient 3 and 4. Presumably this is a bathroom-related event wherein bodily fluids from Patient 1 came into contact with patient 3 or 4, or aerosol/droplet-based transmission in common walking routes to the bathrom. Patient 6 is a 14 year old female, with no blood relation to patient 1, yet she still contracted the virus. Did she give a kiss on the cheek or hug patient 1 or talk to him at length at the party? Or just dumb luck.
Patient 2 got the infection at the birthday party and later died. His wife fell ill and at patient 2’s wake, 10 people fell ill with ANDV 14-40 days after the wake. Droplets and/or aerosols are the most plausible explanation. 82 health care workers were exposed to ANDV-positive patients and performed many high-risk medical procedures (e.g., intubation, cleaning bodily fluids) yet none of them contracted ANDV. That is quite remarkable given that only a small number used any sort of personal protective equipment. In contrast, if this was the seasonal flu or SARS-CoV-2, many of them would have picked up the illness.
There is evidence of droplet or aerosol transmission:
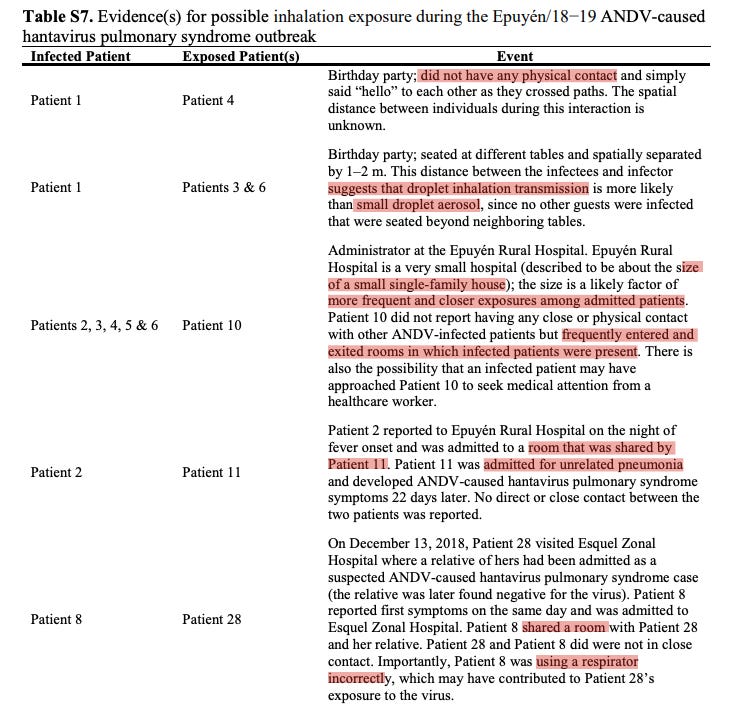
Droplets refer to respiratory particles greater than 5 micrometers in diameter whereas aerosols refer to those less than 5 micrometers in diameter. Droplets are heavier and gravity causes them to settle often within 6 feet of the source. Aerosols can travel long distances, get carried by air current, and stay in the air for hours. The distance at which ANDV can infect others is related to the distribution of respiratory particle sizes that house ANDV. At present, we do not have a good understanding of this distribution and therefore are unsure of the relative importance of aerosol and droplet-based transmission.
What happened to all the patients? 11 died but 68% (n = 23) survived. Further, 44% (15 of 34) were mild cases and all of them survived. Mild means that only supplemental oxygen via nasal cannula or non-invasive ventilation was necessary for recovery. Here is the ventilation requirements and relevant supportive treatment given for each of the 33 patients in Argentina along with the outcomes.
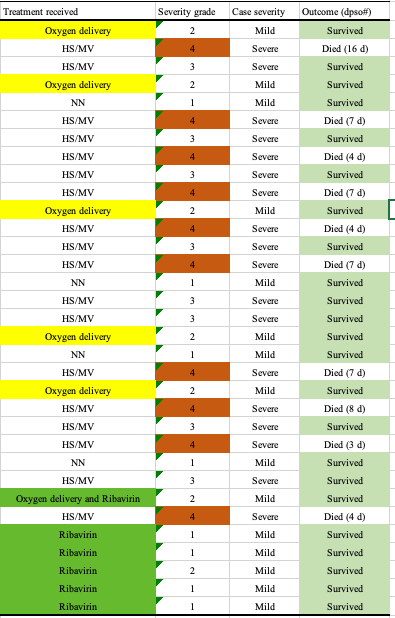
Interestingly, six patients (patients 28, 30–34) received ribavirin7 starting at the first day of fever and all of them survived with mild disease. It is unclear why or how these patients were selected. Or why the 29th patient did not have ribavirin listed in the treatment column in the above chart. There is some thought that ribavirin could be used for post-exposure prophylaxis of high-risk contacts. It appears, on the basis of this study, that if ribavirin is tolerable, on the day of fever onset if ANDV is suspected, initiating ribavirin may be of some help. Unless ribavirin-related toxicities are observed, a patient with ANDV probably does not experience harm if ribavirin is initiated on top of physician-directed medical therapy.
The authors of the NEJM piece also reported the most abnormal laboratory values for each patient. Below are the distributions of those values stratified by those who died and those who did not:

And, by those who experienced severe and mild disease:

I do not see anything obviously different between the groups except for:
lower minimum platelet count in severe disease patients
higher LDH in those who died, and those with severe disease
It’s hard to make anything of this because these are the most extreme values for each patient. One observation reported in the paper is that:
Patients with higher ALT levels and more severe thrombocytopenia were also more likely to be super-spreaders (odds ratio for high ALT level, 1.6; 95% CI, 1.1 to 2.7; odds ratio for low platelet count, 2.9; 95% CI, 1.2 to 13.2)
Among the first 18 patients with confirmed infection (who had not yet been isolated), those with higher viral loads were more likely to spread infection to another person (odds ratio for elevated viral load, 1.7; 95% CI, 1.2 to 3.6).
These results “suggest that person-to-person spread was related to a high viral load and more compromised liver function in the infected patient”.
What about the individuals who died? We have information from a subset of these patients. Patient 2 had gastric cancer and was found to have bone marrow infiltrates related to his gastric cancer at the time of ANDV-hospitalization. He died. Patient 8 was recovering from pneumonia. They died. Patient 10 had a chronic asthmatic condition. They died. Patient 1 and 9 both lived and were in good health prior to infection. Patient 11 was recovering from pneumonia and lived. Patient 3 was otherwise healthy but found to have EBV during ANDV hospitalization. He lived. It appears that an ANDV-positive individual’s probability of survival is porportional to their pre-infection health status.8 We do not have health information on the remaining 24 patients, so it is hard to make any real conclusion specific to ANDV based on this incomplete data.
Lastly, for those interested in prevention measures:
Standard chlorox wipes work on ANDV. These viruses are less stable than other enveloped viruses making them rather susceptible to disinfection wipes and time of exposure to wipes are recommended to be around 30 seconds.
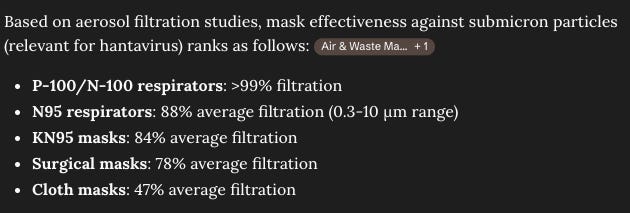
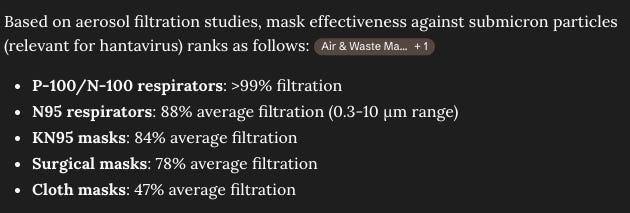
Surgical masks and KN95 masks likely do a decenr job at limiting exposure to ANDV (source 1, source 2):
There are no vaccines for ANDV but there is phase 1 DNA vaccine data and preclinical data from moderna.
Treatment-wise, there is early data showing that plasma from ANDV survivors may curb mortality and there are preclinical data demonstrating the efficacy of antibodies against ANDV (source 1, source 2, source 3)
I will close with an excerpt from a piece written in 1994 about hantavirus infections in North America:
We, in America, are not isolated from what happens in the rest of the world. We must maintain an interest in whatever occurs in remote areas of the world.
Hantaviruses are enveloped, negative-sense single-stranded RNA viruses.
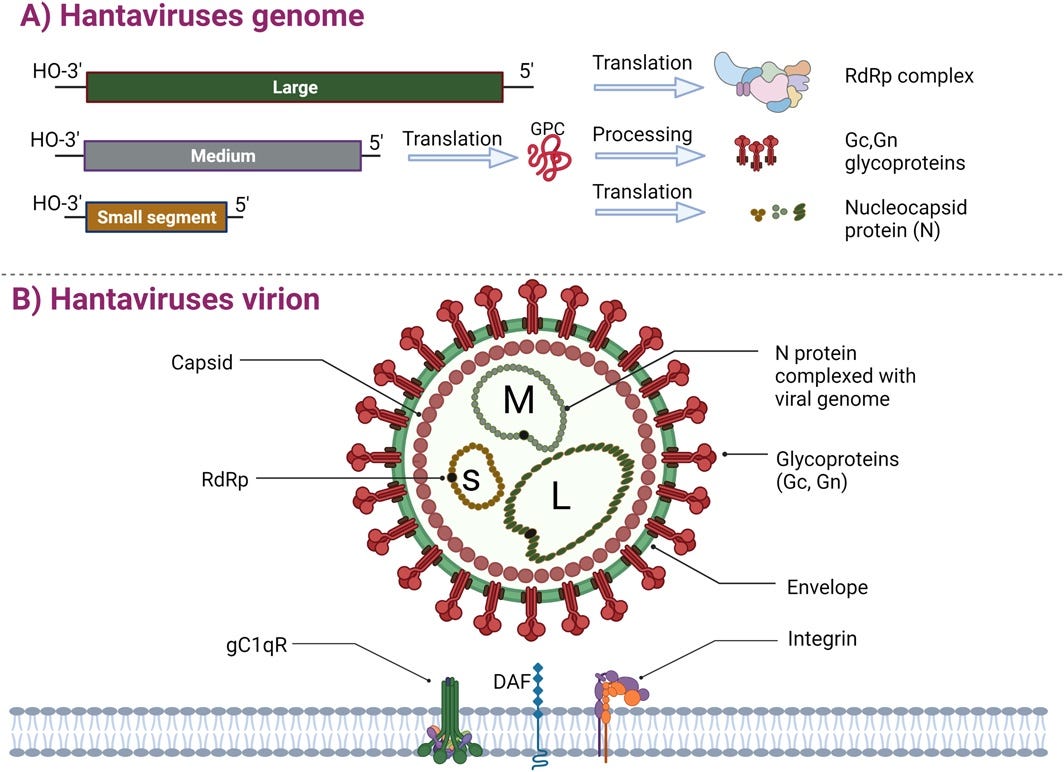
The hantavirus genome has three segments: large (L), medium (M) and small (S) which encode the RNA-dependent RNA polymerase, glycoprotein precursor (that forms Gc and Gn), and nucleocapsid proteins, respectively. In total, Hantavirus genomes encode five proteins, among the most minimally encoded enveloped viruses. The envelope is derived from host cell membranes and is studded with Gn-Gc spike complexes. The spike complexes mediate host cell recognition and entry into cells. Once in cells, the nucleocapsid protein and RNA-polymerase get to work to replicate. ANDV follows this pattern. It has some differences, but that is out of scope for our purposes.
One avenue of investigation is to try to computationally guess at what the sequence differences between Hondius and Epuyen translate into clinically. Particularly, we are interested in transmisability. Therefore, we can attempt to understand how the structure of the surface glycoproteins change as a function of the sequence differences. Then, we can model binding to cell surface receptors that these glycoproteins (PCDH1 and integrin αvβ3). Comparing binding to Epuyen will offer a prediction into how much more or less transmissible Hondius could be.
Patients were typically admitted to the hospital 4d after the onset of prodromal symptoms (e.g., flu-like symptoms) often after two to four outpatient visits. Given the bodily fluid positivity rates, the lack of early recognition poses a risk of infection to health care workers.
This rodent study is by no means direct evidence of aerosol versus droplet transmission. We would need measurements of respiratory particles from ANDV patients to assess this.
It does not mean that an epidemic is certain or that a pandemic will occur.
Here is a tool to understand how many cases and deaths can be expected based on different assumptions of R₀, initial cases, incubation period, control measures, and population at risk. Using pre-control Epuyén/18−19 R₀, no control measures, 11 initial cases, incubation period of 23 days, and 5000 susceptible individuals, we can expect 268 cases and 86 deaths.
Ribavirin is a broad spectrum antiviral that works against RNA viruses. It is used in chronic Hepatitis C, Hepatitis E, and sometimes as a resort of last measure against viral hemorrhagic fever syndromes (e.g., Lassa fever). Its major side effect beyond being a known teratogen is that it causes dose-dependent hemolytic anemia.
This is a generally true finding of basically any biological disease process