
Trying to understand the Bundibugyo Ebola virus (and profiling what we do NOT know)
Clinical course, management, personal prevention strategies, epidemiology

Estimating case fatality rates and reproductive number of the Ebola virus
2026 BDBV Sequence Similarity to 2007 and 2012 BDBV outbreaks
Extent of the Outbreak and Historical Context
The Bundibugyo strain of the Ebola virus is spreading through central Africa. It likely started in late April 2026. As of May 29, per the WHO, there are 906 suspected cases and 223 deaths from those suspected cases. There are 134 confirmed cases: 125 in the Democratic Republic of Congo (DRC) and 9 in Uganda. 18 total deaths amongst confirmed cases. At least three of the confirmed cases in Uganda were from individuals who traveled to DRC and Uganda as of May 27 has closed their border with the DRC. The US is sending citizens who have been exposed to the virus to other countries for observation and treatment which resulted in a handful of Americans being sent to Germany and Czech Republic, including one who tested positive. Non-citizens who have been in DRC, South Sudan, or Uganda in the previous 21 days are not allowed to come to the US. If you are wondering why 21 was selected, it is because the estimated upper bound of the incubation period for Bundibugyo Ebola virus is 21 days.
I recently wrote about the ongoing 2026 Hantavirus outbreak, and many of the general principles covered there will be useful for thinking about this situation. I would recommend following the Brown pandemic report for easy-to-follow and accurate updates on the Ebola virus (thanks to Benjy Renton for initially making me aware of this resource).
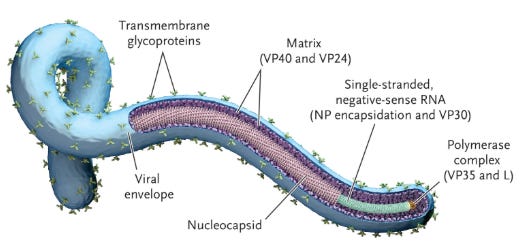
The Ebola virus, shown above, is part of the filovirus family. Critically, there are four species that can infect humans: Zaire ebolavirus (EBOV), Sudan ebolavirus (SUDV), Bundibugyo ebolavirus (BDBV), and Taï Forest ebolavirus (TAFV). In the last 15 years, the Ebola outbreaks have been Zaire or Sudan virus outbreaks. This is the first time Ebola due to BDBV has caused a substantial outbreak. There were much smaller outbreaks in Uganda in 2007 and DRC in 2012.
The scale of what we are seeing today has been observed before. This outbreak is large and moving very fast but not unprecedented once-in-a-hundred-years fast. Here are some charts of confirmed Ebola cases per week in past outbreaks:
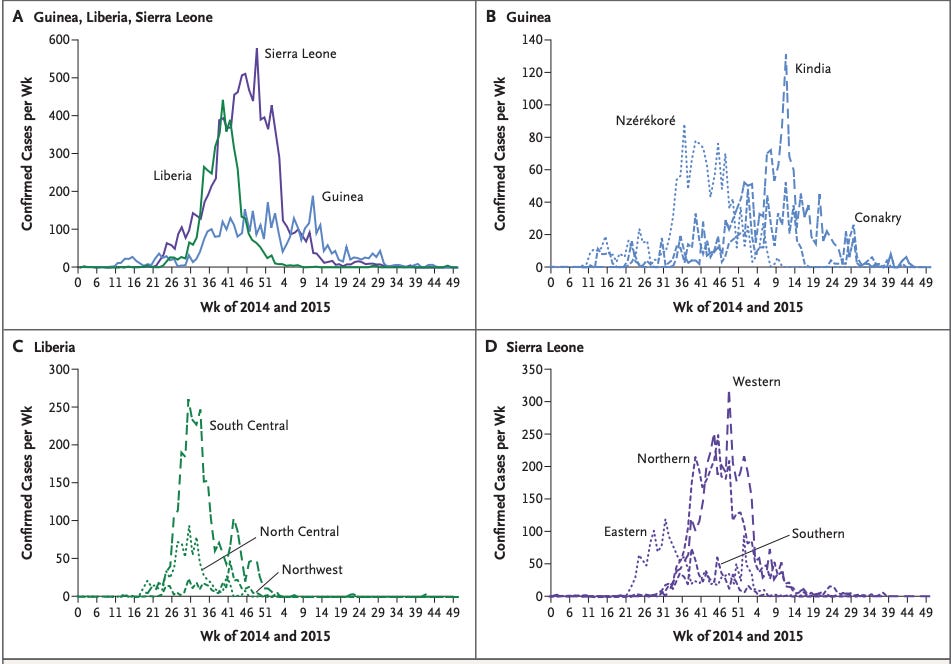
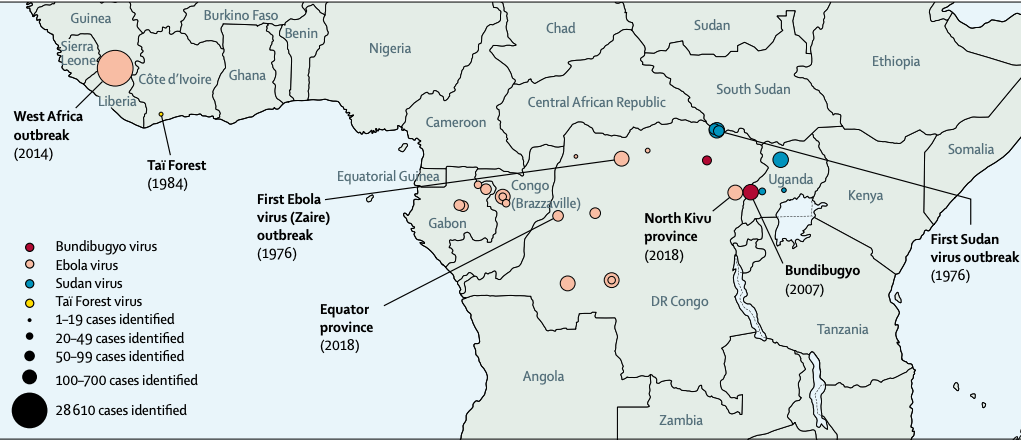
Over a 4-week period, there have been well over 1000 cases in the past. Put differently, here we can see the identified cases in past outbreaks tagged by the species of Ebola that caused it:
Now that we have established that this outbreak is not COVID-19 level of unprecedented, we can try to estimate how lethal and infectious it is. Namely, we are interested in the case fatality rate (CFR) and the reproductive number (R0).
Estimating case fatality rates and reproductive number of the Ebola virus
Both of these measures require an estimate of the total number of cases, and in Ebola outbreaks, we never have a sense of the actual size of the outbreak. Testing is not widespread due to many factors including lack of testing infrastructure and protocol for testing people. Further, for CFR, if people recover on their own without presenting for testing or die with Ebola without ever being tested, we are going to end up with a biased estimate. Now, reasoning through this, I would anticipate that those who are mildly ill then recover get tested less often than those who become severely ill simply because those who become severely ill are more likely to end up interacting with hospitals where testing can be performed. This means that CFRs reported from confirmed counts will be higher than the true CFR. The reproductive number (R0) is the number of secondary cases that a primary case will generate (i.e., how many people will one sick person get sick?). Similar to CFR, due to lack of widespread testing and variability in extent of testing during each outbreak, estimates often have wide ranges or vary widely between outbreaks.
With those caveats, here is a chart of the point estimates for CFR and R0 for many different EBOV and SDUV outbreaks:
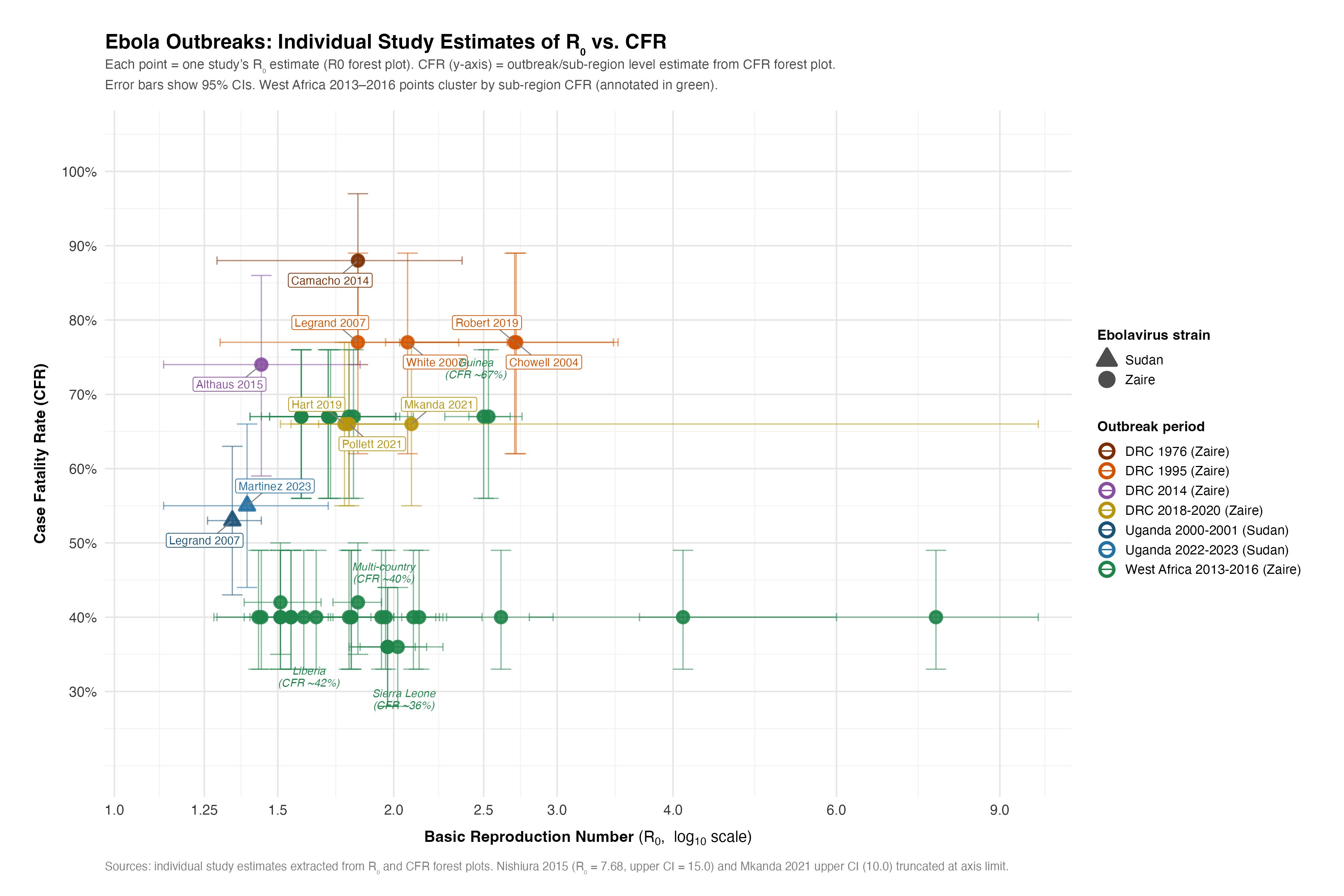
The bottom line is that outbreaks have wide ranges of CFR and R0. Unlike COVID and most aerosol-spread viruses, Ebola does not have lower mortality rates when the R0 goes up. This is also generally true of vector-borne diseases, waterborne infections, and hemorrahagic fevers at large. One reason is that Ebola is able to be spread from people who are deceased. Burial practices or non-sterile handling of the deceased have led to transmission. This also allows for the number of secondary cases that a primary cases can cause to be higher than anticipated. In all, there appears to be a modest positive relationship between mortality rate and R0 based on the Ebola data above.
A Lancet paper estimates the CFR at 25% for Bundibugyo virus disease, 50% for Sudan virus disease, and 80% for Ebola virus disease. This is generally concordant with other estimates but should not be taken as certainty because there is extensive variability amongst estimates. However, BDBV appears to be less deadly than Zaire and Sudan ebola viruses.
Clinical Course of Ebola
In general, after the onset of non-specific viral symptoms (e.g., fever, body aches, fatigue), it produces vomiting and diarrhea that can lead to profound volume and electrolyte loss on the order of 5-10 liters per day. Bleeding from the GI tract, subconjunctival space, or from IV catheter placement sites occur in about half of patients. A secondary consequence either from the virus and/or the volume and electrolyte loss is shock and multi-organ dysfunction. Sepsis, and disseminated intravascular coagulation may follow. Sometimes throat pain, oral ulcers, and difficulty swallowing is observed late in the disease course. The mortality rate varies based on the outbreak and the type of Ebola virus but ranges anywhere from 20%-90%.
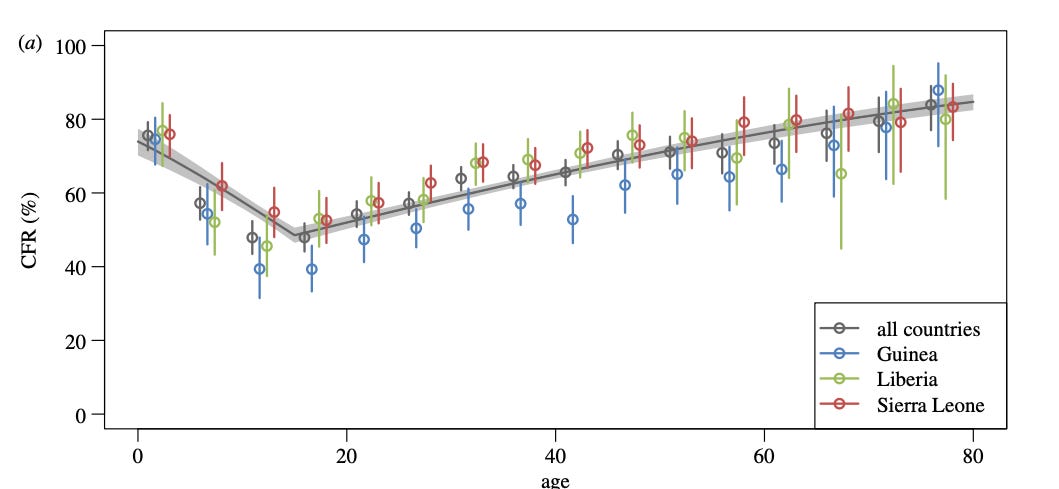
There appears to be a bimodal relationship between age and probability of death due to Ebola. The very young and the very old have higher odds than those in between. And, often those on the younger end of that middle spectrum loosely defined as those aged 10-65 tend to have a lower fatality rate.
Two other prognostic factors emerge across reports of past outbreaks: 1) the faster patients come to the hospital, the greater their chance of survival appears to be, and 2) the lower a patient’s viral load on admission1, the greater their chance of survival appears to be. At face value, it appears that those who come earlier in their disease course and with less severe disease do better. This may be helpful since it leads to faster initiation of supportive therapies (e.g., fluid and electrolyte replacement), and monitoring for escalation of care (e.g., bleeding evaluation).
But, it could be confounded by shared characteristics of those who present earlier or with less severe disease. One example is that these individuals may have better access to health resources, engage in pro-health behaviors at higher rates, and better manage their comorbidities and overall health status. From a case series of patients treated in the US and Europe with Ebola, there is a trend that survivors tend to be younger and have less comorbidities.
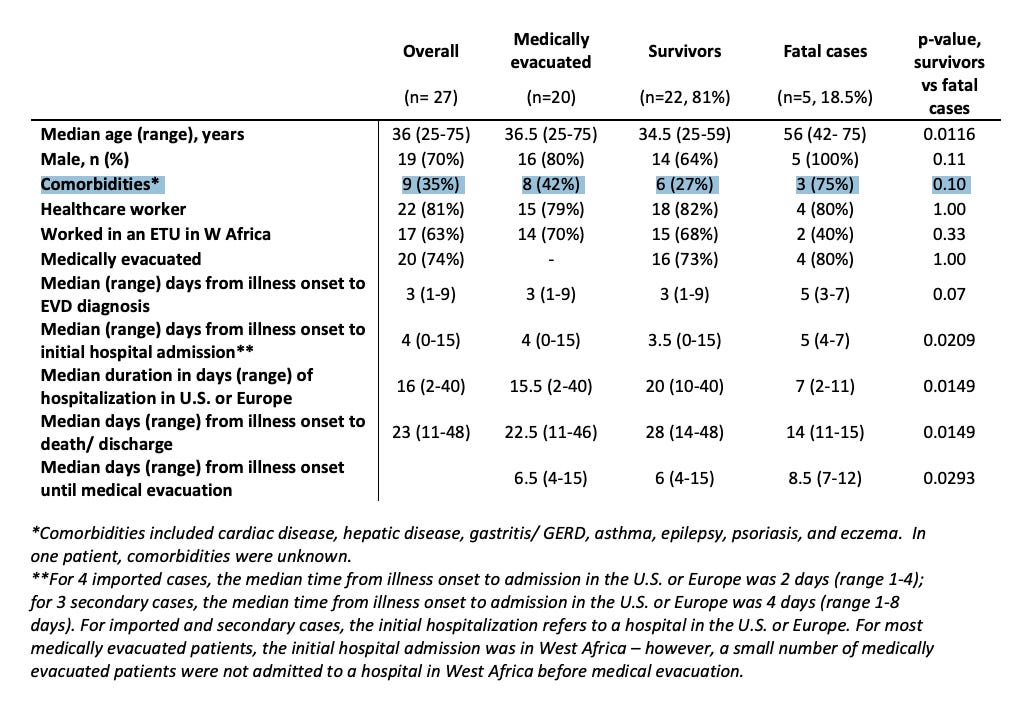
Notice that only 27% of survivors had pre-existing comorbidities but 75% of patients who ultimately died had cardiac disease, hepatic disease, gastritis, asthma, epilepsy, psoriasis and/or eczema.
Other than this table, I could not find much data detailing the comorbidities of the patients along with their Ebola trajectories and so it is hard to understand the impact that physiologic reserve and baseline health status have on fatality. Though, I’d suspect that the more healthy one is at baseline, the better they will do. Another consideration is that ~20% of patients in the case series I read were found to be positive for malaria at the time of admission for their Ebola. It is unclear to me how being malaria-positive affects one’s clinical course with Ebola, but I would guess that it is not helping and could compromise the patient from mounting an adequate response or being able to handle the brunt of the Ebola infection.
Management of Ebola
Mortality for patients with Ebola cared for in Africa ranged from 37%-74%. However, mortality for patients with Ebola cared for in the US or Europe was 19% (caveat: much smaller sample size of n = 27). Why could this be the case? The fundamental disease biology is the same, yet the outcomes are very different. In Africa, the majority of patients with Ebola are treated in centers vastly under-equipped than those in America and Europe. Here is a quote from the 2012 paper describing the data collection in Uganda for patients with BDBV:
Of the ten patients whose axillary body temperature was recorded at least once during hospitalisation, five (50%) had their temperature recorded at least once daily for 80% of their stay, while seven (70%) had their temperature recorded at least once daily for 50% of their stay (data not shown). Heart rate, respiratory rate, and blood pressure were not recorded for any patients
This means that most vitals were not recorded and temperature was recorded once a day for half of patients. ICU patients admitted to academic centers in the US are watched much more closely. We can only act to correct or treat things if we understand them to be off or heading in the wrong direction. Therefore, the lack of vital monitoring serves as a marker for the extent of care that these centers were able to provide in 2012 in Uganda. Of course, things have changed and progressed since then, but this is a point worth considering when trying to understand why CFRs historically have been different between geographies.
Intensive care units at academic medical centers in the United States and Europe have a lot more resources. Those extra resources afford the opportunity to better support patients (e.g., continuous renal replacement therapy, invasive ventilation, etc.). One of the key lessons from the two-patient case series of Zaire strain Ebola, where both patients lived, is the need for attentive and careful electrolyte and volume replacement. In general, there are two main things that will kill you with Ebola: 1) Ebola itself, 2) the volume and electrolyte loss. And, while we cannot treat the former, we can try to prevent the latter from wreaking havoc.
Since Ebola results in electrolyte and volume loss, we ought to replace what was lost within reason. Fluid management in the clinical setting is an art and the subject of much discussion so I won’t try to summarize it here. But, it is worth highlighting that Ebola often leads to severe diarrhea (over vomiting) and excess diarrhea can lead to hypokalemia, hyponatremia, hypomagnesemia, hypocalcemia, and sometimes hypoglycemia. So, we must monitor and replace as necessary because electrolyte derangements can be life threatening on their own.2 For example, hypokalemia can lead to serious cardiac arrhythmias and subsequent sudden cardiac death. Also, generic oral sports drinks like Gatorade should be avoided in severe diarrhea because they do not contain the right mix of electrolytes and sugar (e.g., too little potassium, too much sugar) which can make the problem worse and can give a false sense of comfort. Instead, pedialyte or other balanced oral rehydration solutions are recommended. If not tolerated, IV isotonic crystalloid is a good choice.3
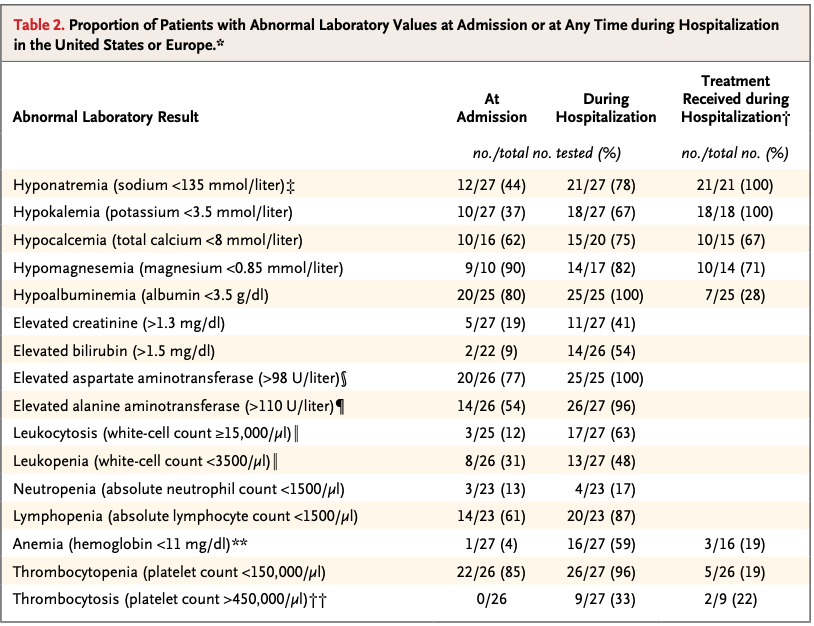
We can observe that serious electrolyte abnormalities were standard. Median maximum stool discharge per 24 hours was 3000 mL. That is cholera-esque and that level of diarrhea will lead to electrolyte abnormalities. About 50% had signs of bleeding but only 7% had gross hemorrhage at any time. 85% of patients were managed without invasive ventilation. 5 of the 27 patients died and the median age of those who died was 56 versus 35 for those who lived. Up to 41% of people could have died if advanced organ support had been unavailable (e.g., invasive ventilation and CRRT).
Often times, patients with ebola experience vascular leak and/or renal impairment due to the virus or its sequelae which means that if too aggressive of replacement is pursued, we will third space a lot of the fluid leading to a tremendous amount of edema and further organ dysfunction. Also, patients may lose vital proteins (e.g., albumin and caogulation factors). The vascular leak may be better managed by use of specific fluid solutions including albumin containing fluids though data is limited on this and crystalloid tends to be the default choice.
The majority also received experimental therapies. It is unclear if convalescent plasma from Ebola survivors or experimental monoclonal antibodies help in recovery, but, so long as it is not harmful (which was not overtly observed in this study), it is worth the effort given the seriousness of this disease. The question is when to offer such therapies in a patient’s clinical course because they are not proven to work and do come with side effects. It would be unnecessary and perhaps cause more problems for a patient who will never go on to develop severe disease, loosely defined as that requiring ICU-level care.
BDBV Clinical Course
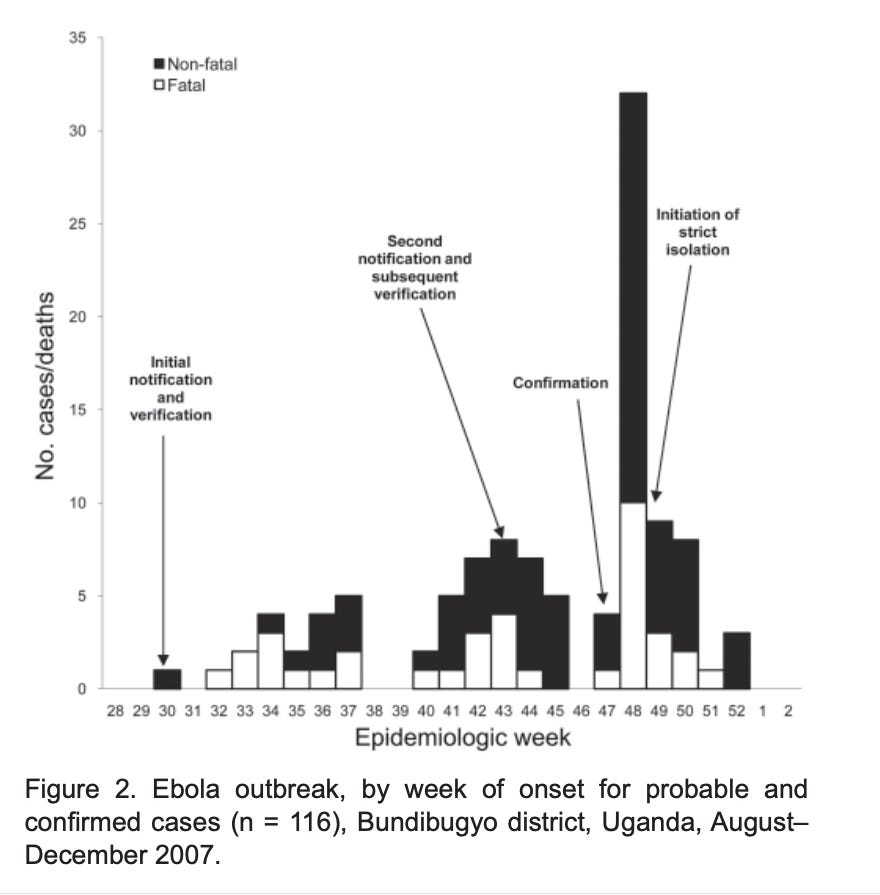
We have data from a paper describing 93 probable cases, 56 lab-confirmed cases, and 37 deaths (CFR 25%) in Uganda in 2007. CFR was 33% amongst confirmed cases. And another from the DRC in 2012 describing 36 confirmed, 21 probable and 5 suspect cases, including 34 fatalities (CFR 55%). The clinical syndrome is largely the same as described above. Individuals who received oral rehydration and other supportive therapies had a 40% lower fatality rate.
We can see the distribution of fatal outcomes as a function of time and measures implemented during the 2007 outbreak:
Patients in these outbreaks were often given antimalarials and antibiotics at time of presentation given the limited ability to process biological samples for alternative diagnoses. I imagine that there is some negative cost to the patient if the patient has Ebola but no malaria or bacterial infection yet they are given antimalarials and/or antibacterials if only because no treatment comes without a side effect.
We have no treatments or vaccines specific to BDBV besides supportive care.
BDBV incubation period and precautions
Incubation period is between 1-21 days for BDBV with a median of 7 days. We do not have BDBV specific data on tissue positivity data. But, we do for EBOV (Zaire Ebola):
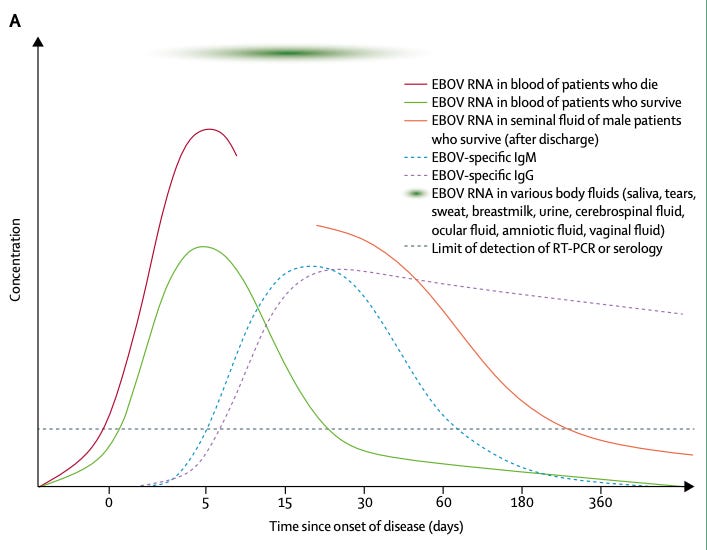
We can observe that Ebola RNA lives in blood, tears, urine, sweat, and can persist in immunologically preserved sites like testes, eyes, and the central nervous system. Further, there is evidence that asymptomatic individuals are capable of transmitting the virus.
Right about now you might be wondering where the Ebola virus comes from. And, to the best of our knowledge, we think fruit bats are the natural host but we have yet to isolate the virus from these animals. Occasional spillovers to humans and apes are thought to occur. Human-to-human transmission occurs by direct contact with bodily fluids from infected humans. Specifically, direct contact of infected bodily fluids including sweat with broken skin or mucous membranes (e.g., lips, eyes).
So, how do we prevent the spread of Ebola? What can an individual who does not want to get Ebola do? They can try to cover broken skin and their mucous membranes. Perhaps with masks or eyeglasses and full-length clothing. But, it is not substitute for full personal protective equipment. Second, how can one clean their surroundings to be “Ebola-free”. The short answer is that over-the-counter bleach and Chlorox wipes work on non-porous surfaces but require 2.5-5 minutes of contact time [source 1, source 2, source 3, source 4]. 4

2026 BDBV Sequence Similarity to 2007 and 2012 BDBV outbreaks
Excellent work out of DRC resulted in BDBV sequences from 2026 cases being deposited online. And, basically, the cases sequenced from the 2026 outbreak are very similar to previous outbreaks. Note that 2026 is in red, 2007 is in yellow and 2012 is in blue.
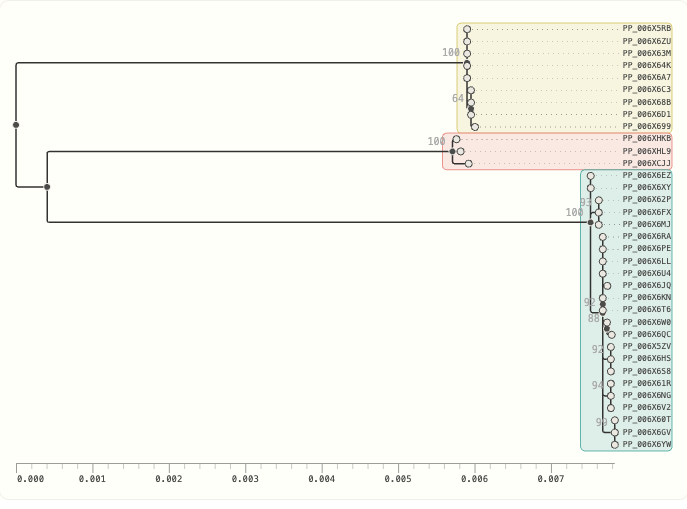
I am no virologist but we can observe that from a common point on the far left, the current outbreak samples live between the 2007 and 2012. This implies that we are not seeing some novel BDBV variant with truly out-of-left-field properties. This also suggests that what we know about BDBV in the past is likely to hold for the ongoing situation.
Vaccines and emerging treatment measures
Ebola is a negative-sene single-stranded RNA virus of the family Filoviridae. Ebola vaccines target the surface glycoproteins responsible for mediating entry into cells.
We have a vaccine against the Zaire strain of the Ebola virus but it will not cover you against BDBV. And, we have no vaccines for BDBV. Moderna, the University of Oxford, and IAVI are working on a vaccine. Soligenix and Geovax have commented that they could use their vaccine platforms to make BDBV vaccines if funded.
Post-Ebola syndrome
Individuals who survive Ebola at the time of discharge report weakness, weight loss, abnormal lab results, and anemia. Other papers report symptom burden amongst survivors including persistent arthralgia, vision-threatening uveitis, and deleterious effects on mental health. This is to say that surviving Ebola means not dying of it and recovery back to baseline health status is not guaranteed and will take time.
Another finding is that lower viral loads during infection translate to lower mortality. This is a nice confirmatory finding because it would be more alarming to find that death is equally likely regardless of viral load. But, we expect lower viral loads to lead to lower mortality because it means that the patient’s body is handling the infection better.
So, tailoring the rehydration plan to have enough potassium, magnesium, and calcium is necessary. And, monitoring blood glucose and treating based on results.
There are MANY different IV fluids and this is the subject of much discussion, opinion, trials, and clinical evidence papers. I will not attempt to cover this in the post and leave that as an exploration for the reader.
My opinion is that something is better than nothing and if you think you are concerned about exposure, for example on a flight in the region or through a major airport, a mask and wiping down of surfaces followed by washing your airport clothes when you get home is reasonable and probably not too much of a burden.